
This blog was originally published by Health Affairs on February 2, 2018.
Community-based organizations such as area agencies on aging (AAAs) and centers for independent living (CILs) have served for decades as cost-effective, trusted, and proven resources for addressing the health-related social needs of older adults and people with disabilities, including long-term care needs. Yet, until recently, the health care sector has had little awareness of the value of these home and community-based resources. AAAs and other community-based organizations have typically relied on traditional funding sources such as the Older Americans Act of 1965. However, these funds have remained flat or declined, despite upward growth in the number of people—older adults and people with disabilities living in the community—who could benefit from community-based organizations’ support (Exhibit 1).
Exhibit 1: Older Americans Act Funding, Medicare Spending, And Older Adult Population Growth
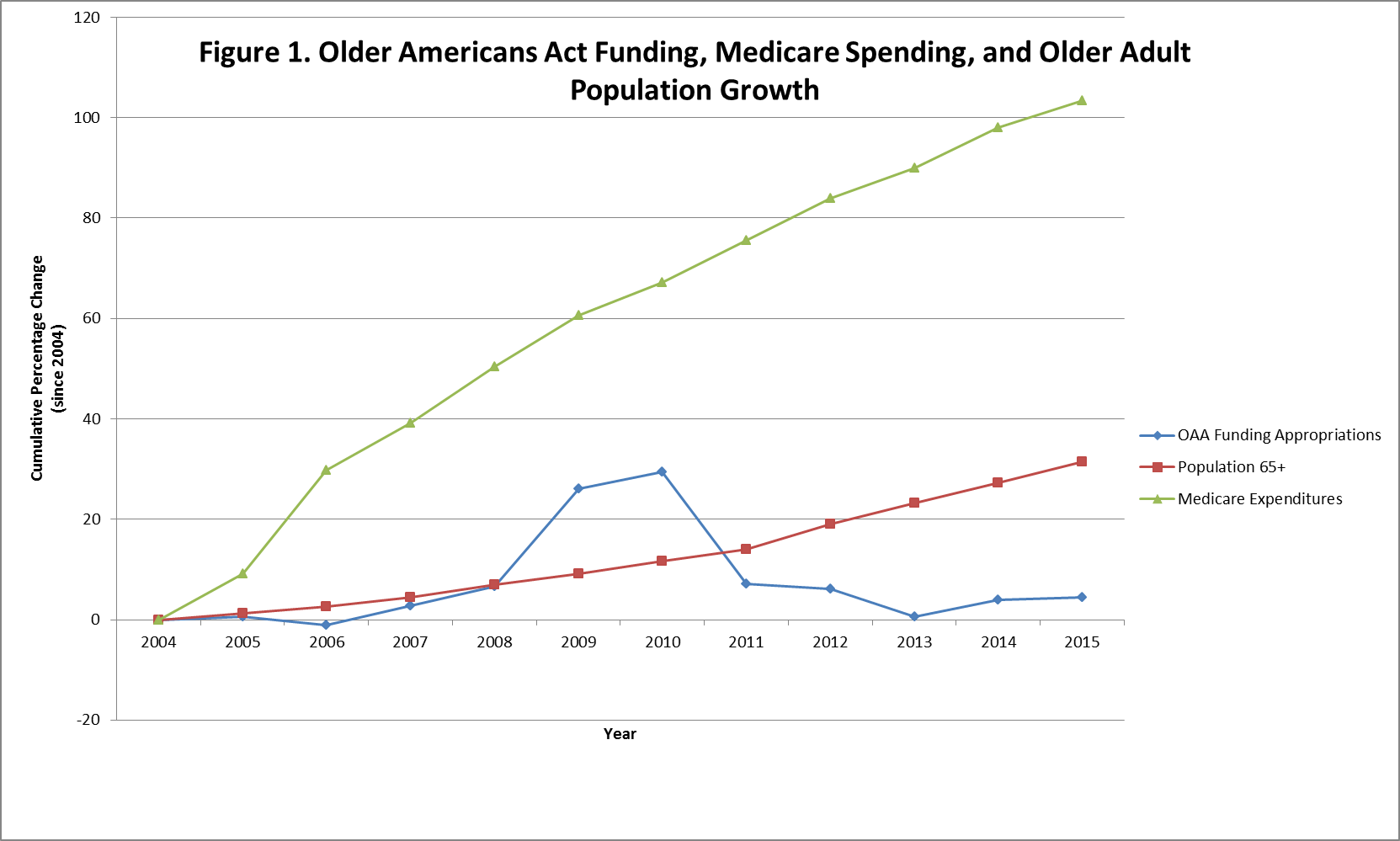
Source: Adapted from Parikh RB, Montgomery A, Lynn J. The Older Americans Act at 50—community-based care in a value-driven era. N Engl J Med. 2015;373(5):399-401. Values have not been adjusted for inflation.
Medicare spending has also steadily increased over the past decades. At the same time, there is a growing recognition of evidence showing that the majority of health care costs are driven by factors outside of the clinical environment including the social determinants of health such as food security, housing instability and quality, and utility and transportation access. There is additional evidence showing that functional limitations are associated with higher Medicare costs. Together, these factors have created new incentives for health care entities and community-based organizations to partner to optimize efficient and effective integrated care for older adults and people with disabilities.
Early Evidence
These partnerships appear to be having a positive impact. In the January 2018 issue of Health Affairs, researchers from Yale University and the Scripps Gerontology Center at Miami University of Ohio published a study finding that AAA involvement in a broad variety of cross-sector collaborations with health care and social service organizations is associated with a reduction in hospital re-admission rates. The study also found that counties in which AAAs had nursing home diversion programs had significantly lower avoidable nursing home use rates. The authors conclude that their “findings…highlight [AAAs] as a promising potential source of leadership in convening cross-sectoral partnerships to improve health for older adults.”
Community-based organizations such as AAAs that work directly with individuals in their homes and communities have demonstrated experience in addressing issues that are beyond the traditional reach of clinicians. Community-based organizations can identify and address risk factors, such as poor self-care skills, environmental hazards, need for social supports or protection, mental health challenges, or difficulty with medication management that can have a significant impact on health and health care spending. Medicaid managed long-term services and supports programs and other demonstration programs have shown that integrating health care and social supports can be highly effective in helping individuals remain in the community, which is where 90 percent of older adults prefer to stay as they age. In addition, a 2017 survey of 12 states with Medicaid managed long-term services and supports programs found that states have experienced sharp reductions in long-term nursing home stays and hospitalizations.
Several studies have found that home-delivered meals provided by community-based organizations improve health and are associated with reduced nursing home use in older adults with low-care needs. Other research has demonstrated the impact of food insecurity on health and health care spending. For example, one study found that older adults on Medicaid in Maryland were 14 percent less likely to be hospitalized and 23 percent less likely to enter a nursing home in the following year if they were enrolled in the Supplemental Nutrition Assistance Program. Results of a recent study also demonstrate that states with a higher ratio of social services to health spending showed better health outcomes on measures such as the number of days with activity limitations in the past 30 days and mortality rates for type 2 diabetes, lung cancer and heart attack.
The Aging and Disability Business Institute Survey On Community-Based Organization Contracts With Health Care Partners
To respond to the growing demand for their services in the evolving health care marketplace, community-based organizations have been increasing their business acumen and organizational capacity. Building on several years of support from the John A. Hartford Foundation, the US Administration for Community Living, the SCAN Foundation, the Gary and Mary West Foundation, the Colorado Health Foundation, and the Buck Family Fund of the Marin Community Foundation, the Aging and Disability Business Institute (Business Institute) was created in April 2016 to successfully build and strengthen contract-based partnerships between community-based organizations and the health care system. Led by the National Association of Area Agencies on Aging (n4a), in partnership with several leading aging and disability organizations, the Business Institute serves as a national resource center for agencies interested in acquiring skills for sustainability and business planning. As staff for the Business Institute, we provide training and technical assistance to enhance the business capacity of community-based organizations, positioning them to negotiate, secure, and successfully implement contracts with health care entities.
To better understand and track current contracting practices and national trends among community-based organizations, the Business Institute, in partnership with the Scripps Gerontology Center at Miami University, launched a national request for information (RFI) survey in July 2017 to AAAs, CILs, and other community-based organizations. A total of 593 organizations participated in the RFI survey. More than half of all responding community-based organizations either have a contract or are pursuing contracts with health care entities. Currently, 38.1 percent of responding community-based organizations have one or more contracts with a health care entity, with an additional 16.5 percent reporting that they are pursuing at least one contract with a health care entity. Community-based organizations are most frequently contracting with the following payers: Medicaid managed care organizations (35.0 percent), hospital systems (27.8 percent), Veterans Affairs medical centers (19.1 percent), and Medicare-Medicaid duals plans (16.1 percent) (Exhibit 2).
Exhibit 2: Most Common Health Care Partners Engaged With Community-Based Organizations
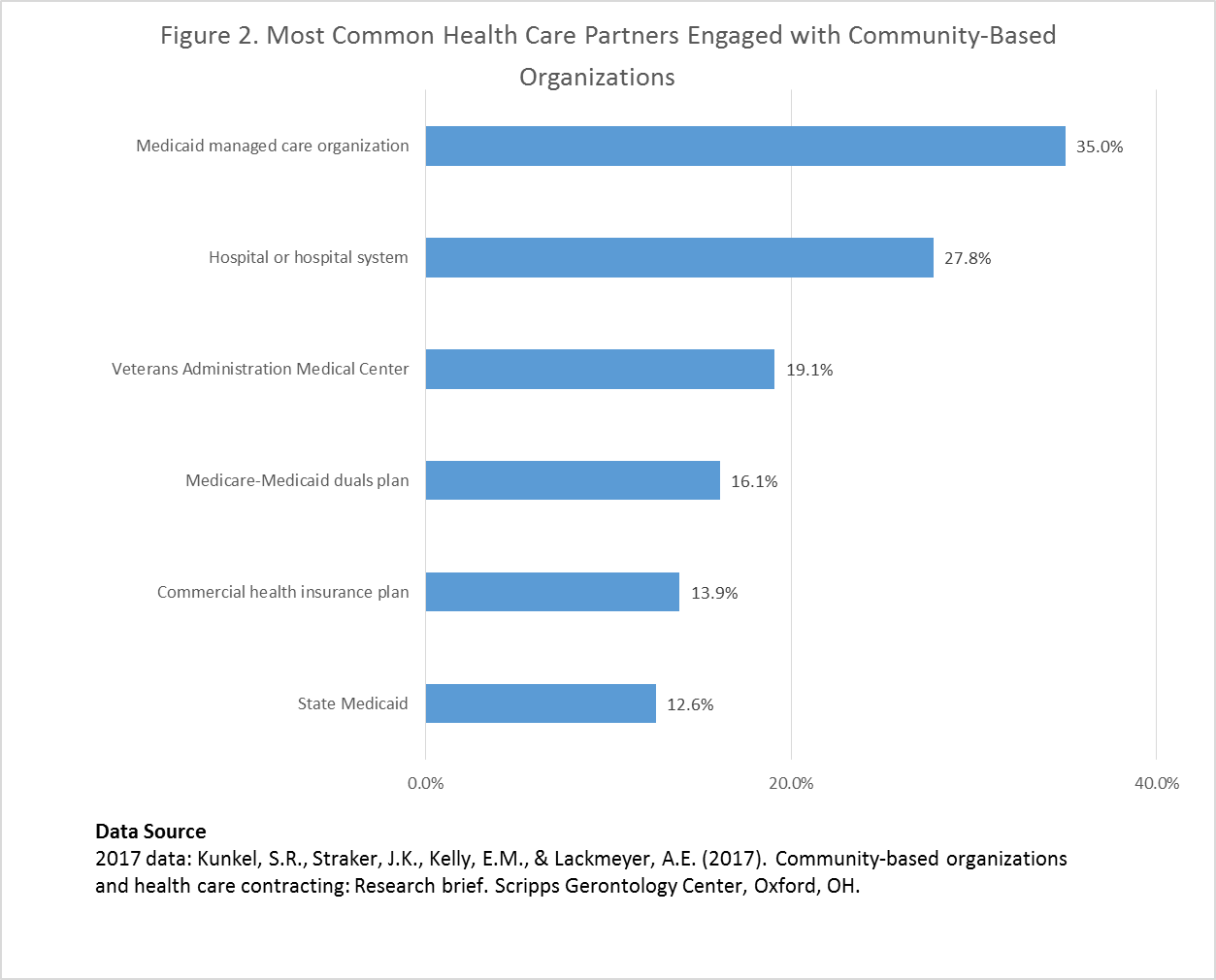
Source: Kunkel SR, Straker JK, Kelly EM, Lackmeyer AE. Community-based organizations and health care contracting: research brief. Oxford (OH): Scripps Gerontology Center; 2017 Dec.
The most common services provided under contracts with these payers suggest that health care entities are engaging community-based organizations for the value they add in addressing the health-related social needs of their most complex and vulnerable patients (Exhibit 3). The RFI results show that nearly half of community-based organizations contracting with health care entities are providing case management (49.3 percent) (for example, care coordination or service coordination). Other common services include care transitions/discharge planning at 29.1 percent, home care (for example, homemaker, personal assistance, personal care) at 26.5 percent, and nutrition services at 26.0 percent. On average, community agencies provide three services per contract.
Exhibit 3: Most Common Services Provided Through Contracts Between Community-Based Organizations And Health Care Entities
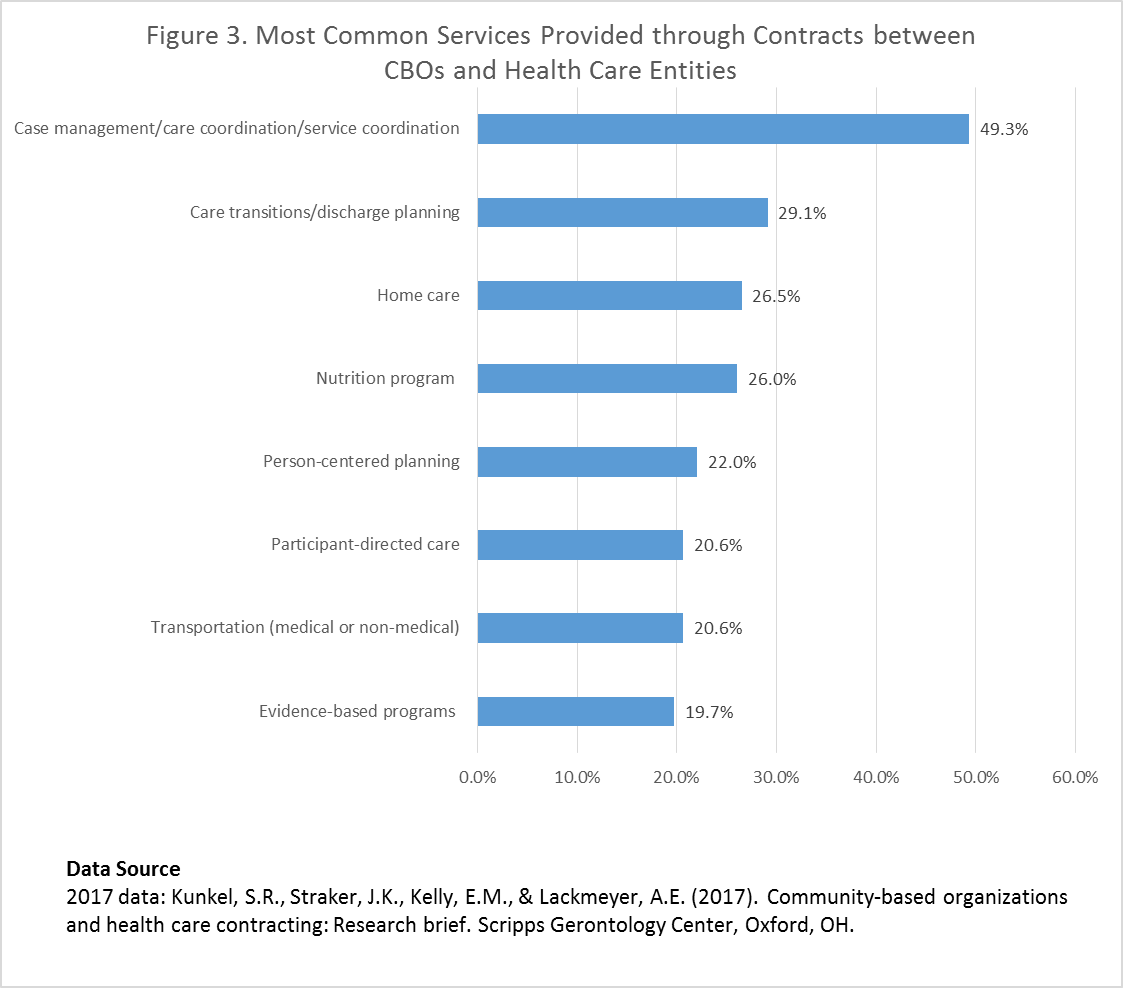
Source: Kunkel SR, Straker JK, Kelly EM, Lackmeyer AE. Community-based organizations and health care contracting: research brief. Oxford (OH): Scripps Gerontology Center; 2017 Dec.
Future Directions For Community-Based Organization And Health Care Partnerships
Our findings indicate that community-based organizations are forming partnerships with health care entities to address health-related social needs—especially in the Medicaid managed care organization and hospital arenas. These findings are consistent with the trends that n4a (in partnership with Scripps Gerontology Center) has documented through a series of surveys of AAAs since 2009. The 2016 survey found that more than 63 percent of AAA survey respondents now participate in at least one integrated care opportunity, up from 55 percent in 2013.
Because of their deep community roots, community-based organizations often have numerous established relationships within the communities they serve and strong expertise in addressing social supports, such as housing, nutrition, transportation, and personal care for older adults and people with disabilities. The health care sector appears to be taking notice.
The shift in the health care system from payment for volume to payment for value has provided additional incentives for providers and payers to work with community-based organizations, both to connect patients with social supports and to help them manage chronic conditions. In addition to experience providing case management and care transitions for complex patients, community-based organizations have broad experience in providing evidence-based disease prevention and health promotion programs for older adults and people with disabilities. A recent survey found that 93 percent of AAAs already provide these aging and disability evidence-based programs. Our RFI results show that for contracting organizations, 19.7 percent provided evidence-based programs through their contracts. Evidence-based programs, such as the Chronic Disease Self-Management Programs, have shown great success in improving health outcomes such as fatigue, pain, and shortness of breath. These programs, which activate people with chronic conditions to better manage their conditions, have potential to have a much wider impact, given that 42 percent of US adults have one or more chronic conditions. As community-based organizations increase their capacity to develop networks and provide services, we expect that partnerships with health care to provide evidence-based programs will continue to grow.
In addition, policy changes at both the state and federal level will likely continue to accelerate these partnership opportunities. More than 20 states are currently offering Medicaid managed long-term services and supports for some or all of their populations and additional states are either currently developing or considering it. The Centers for Medicare and Medicaid Services reports that it has experienced increasing interest from states in the form of concept papers, waiver applications, and requests for technical assistance regarding Medicaid managed long-term services and supports.
At the federal level, the Center for Medicare and Medicaid Innovation (Innovation Center) has developed several models that work toward improving alignment between community-based organizations and the health care sector, such as the Community-Based Care Transitions Program, accountable health communities model and financial alignment initiative for dually eligible beneficiaries. In response to the Innovation Center’s recent request for information, the Business Institute has strongly suggested that further integration of social supports and health care are necessary for a high-quality, person-centered care system for this growing population, and community-based organizations will need to play a central role.
Moreover, the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act, passed in September 2017 by the US Senate, could open up further opportunities for partnerships between Medicare Advantage plans and community-based organizations. The legislation, now awaiting action in the House, would allow Medicare Advantage (MA) plans to provide and target supplementary benefits—including nonhealth-related benefits—to complex beneficiaries. This change could encourage MA plans to partner with community-based organizations to provide services that MA plans have not traditionally offered, such as nutrition services or home care. Policy changes and payment incentives such as these are creating more opportunities for many community-based organizations to establish formal health care partnerships.
Looking Ahead
From the RFI, we know that among agencies currently not pursuing contracts (45.4 percent of respondents), nearly four in 10 (39.4 percent) say they need more information and guidance. Through the technical assistance and educational opportunities offered by the Business Institute, we hope to close this gap. A second round of the RFI, scheduled to go out later this year, will allow us to build upon our understanding of contractual relationships between community-based organizations and health care entities over time. Our goal is to increase awareness of the unique expertise that community-based organizations provide in delivering services to older adults and people with disabilities, while simultaneously providing the community-based organizations the resources and tools they need to be successful.