Recent policy changes indicate a growing recognition that factors called the social determinants of health (SDOH) can play a significant role in an individual’s health and well-being—a fact that community-based aging and disability organizations (CBOs) have long known. The SDOH include access to transportation, healthy food and accessible housing. Research shows that simple, low-cost services and supports that address the SDOH have the potential to help individuals who have complex care needs through improved self-care management, increased adherence to their doctor’s plan of care and the avoidance of unnecessary health care expenses, including hospital admissions and/or institutionalization in nursing homes. For example, according to a recent RAND study as reported by the Centers for Disease Control and Prevention, chronic and mental health conditions contribute to 90 percent of annual health care expenditures in the United States.[1] The study goes on to show that many of these chronic and mental health conditions can be prevented or managed by addressing social and lifestyle factors outside the focus of today’s health care system.[2]
However, the systems we use to deliver, track and finance health care and social services are often siloed, which results in separate structures and financing systems and creating significant challenges for delivering true person-centered care, leaving countless missed opportunities to improve health outcomes and reduce the total cost of care.
The good news is that policymakers are beginning to explore ways to encourage collaboration between managed care plans, health systems and CBOs that have the expertise necessary to help older adults and people with disabilities with service and support needs. Two significant recent developments offer a level of optimism for the future.
CHRONIC Care Act
A promising start to covering services that address the SDOH for Medicare beneficiaries occurred in February 2018 when the Creating High-Quality Results and Outcomes Necessary to Improve Chronic (CHRONIC) Care Act became law as part of the Bipartisan Budget Act of 2018. Commonly referred to as the CHRONIC Care Act, this new law expands the range of supplemental benefits that may be offered by Medicare Advantage (MA) plans, giving these plans greater flexibility in structuring and targeting supplemental benefits that are not “primarily health-related” to chronically ill plan members.
Prior to the CHRONIC Care Act, MA supplemental benefits were required to be primarily health-related, such as dental care and vision benefits, and made available to all plan members regardless of health condition. The CHRONIC Care Act allows MA plans to offer special Supplemental Benefits for the Chronically Ill (SSBCI). These benefits may include services that are not primarily health related, such as home and community-based services that address the SDOH, as long as the services have a reasonable expectation of improving or maintaining the member’s health or overall function. The law also waives the requirement that SSBCI be made available to all members as long as the offering is based on health status or disease state and ensures that similarly situated enrollees are treated the same way.
While SSBCI are a small part of the MA program, the shift to address individual needs, not all of which may be primarily health related, but which may have a significant impact on health and health care utilization, is significant.
2020 Call Letter and Subsequent Guidance
In the 2020 Final Call Letter, which provides guidance to plans on the rules for the coming plan year, and subsequent guidance issued shortly thereafter, the Centers for Medicare & Medicaid Services (CMS) gives MA plans new flexibility to:
• develop services they offer as SSBCI, as long as there is a reasonable expectation of improving and/or maintaining health or overall function;
• target SSBCI as it relates to the individual enrollee’s specific condition and needs;
• address the social determinants of health (SDOH); and
• consider SDOH as one of (but not the sole) factor in targeting benefits.
CMS defines a chronically ill enrollee as an individual who:
• has one or more comorbid and medically complex chronic conditions that is life threatening or significantly limits the overall health or function of the enrollee;
• has a high risk of hospitalization or other adverse health outcomes; and
• requires intensive care coordination.
CMS notes in its 2020 Call Letter that about 73 percent, or nearly 15 million, current MA enrollees qualify as chronically ill and that services that could be covered as SSBCI benefits include pest control, structural home modifications and transportation for non–primarily health related needs.
How Are SSBCI Financed?
MA plans can pay for SSBCI two ways—through their rebate dollars and/or plan premiums. The chart below shows some of the factors that MA plans must consider when developing their plans for the coming year and, specifically, how or why they may choose to include, exclude or limit SSBCI benefits in their plans.

How Are MA Plans Implementing SSBCI?
Improving Outcomes and Reducing Costs. MA plans are looking for ways to provide non-medical services and supports that can help people who have complex care needs improve outcomes and avoid expensive medical care. Given the tremendous variation in these complex care needs, there is no single package of services and supports that will work for everyone.
Testing New Innovations. MA plans see potential in attracting and managing members who have complex care needs and in testing ideas that could impact their overall health outcomes and costs.
Mitigating Risk. MA plans can find value managing care for people with complex care needs but are concerned about the risk of attracting too many members who have high health care costs without having made a sufficient risk adjustment in the premium to account for these costs.
Defining Value. MA plans offering supplemental benefits in 2019 view the offering as a testing ground to determine the value of these new types of benefits and their capacity to target them to a subset of their members.
The supplemental benefits that were included in 2019 MA plan bids were limited and considered by the plans to be a test of the concept, since the plans lacked sufficient data to adequately design and price the benefits. Plans that did include flexible supplemental benefits in their 2019 bids used fairly conservative approaches: limited personal care and homemaker services, meal delivery for members transitioning to the community from institutional settings, adult day services, and non-emergent transportation. Experts expect that many more plans will offer SSBCI in 2020, now that they have more lead time and more guidance on the types of services they can offer.
Barriers to Consider
MA plans have limited financial resources and, as noted above, many unknowns remain with SSBCI. Will the new benefit be popular among plans? Among beneficiaries? Will it lead to improved health and well-being for enrollees receiving the benefits? If the MA plan includes the benefit, is there sufficient provider capacity to ensure the benefits are delivered as promised and with high quality? How will the SSBCI impact claims costs and Medicare’s risk adjustment?
As a result, we expect MA plans to continue to move forward on SSBCI, albeit with caution, as they learn more in the coming years.
The Role of Aging and Disability CBOs
In order to improve the health and well-being of Medicare Advantage enrollees through the implementation of SSBCI, an array of stakeholders, including AAAs and other CBOs, will have to collaborate. Well-prepared CBOs will be critical partners for MA plans as they test SSBCI offerings that address the SDOH.
Unlike Medicaid LTSS health plans, MA plans have not historically maintained networks of non-medical service providers and typically don’t have strong relationships or experience with the CBOs, home care agencies, adult day care centers and other providers that would deliver these services. In the process of deciding on what SSBCI benefits to offer, MA plans must ensure there are service providers in the markets in which the benefits are being offered that can provide it with the scale necessary to serve the MA plan’s entire service area—an opportunity for aging and disability CBOs.
CBOs selected for partnership with MA plans that are testing SSBCI benefit offerings must be able to meet contracting requirements and provide consistent, high-quality services. Some MA plans rely on internal personnel who specialize in vendor contracting. Other MA plans may use an experienced third party to assess the capacity and quality of potential vendors.
Adding to this opportunity is the fact that the 2020 Call Letter specifically mentions CBOs:
“MA coordinated care plans are required to ‘coordinate MA benefits with community and social services generally available in the area served by the MA plan.”
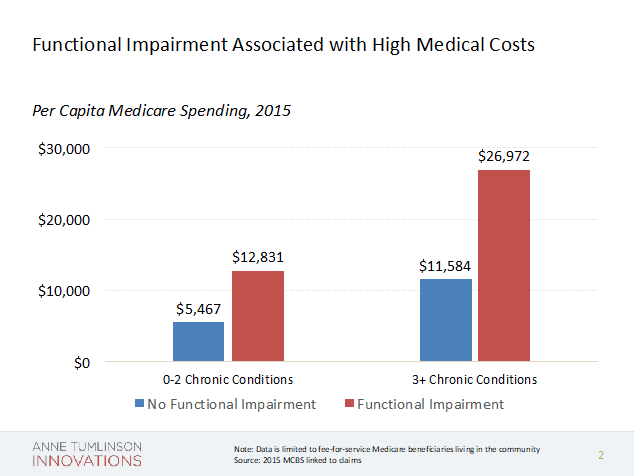
In addition to contracting with MA plans to provide SSBCI, CBOs can also help MA plans determine whether an individual meets the eligibility requirements for SSBCI. A key benefit of MA plans partnering with CBOs is the fact that CBOs have more experience identifying functional limitations, which contribute to higher medical costs than chronic conditions alone.
Conclusion
The inclusion of SSBCI is a significant step toward providing holistic coverage in the Medicare program to more effectively manage chronic conditions and reduce the impact on overall Medicare spending for beneficiaries who have the most complex care needs. These changes create a testing ground for expanded Medicare coverage and the potential to pay for these added benefits through the Medicare savings they generate.
Though SSBCI are expected to be limited in scope over the next few years, MA plans will be testing a wide variety of pilots to learn what works with the most positive results, creating the building blocks for future collaborations. Recent policy changes that allow MA plans to cover factors associated with the social determinants of health—thereby taking steps toward improving the health and well-being of certain chronically ill MA enrollees while reducing costs—represent a sea change. To seize this opportunity, CBOs must position and prepare themselves as partners for MA plans that are embracing these changes.
[1] https://www.cdc.gov/chronicdisease/about/costs/index.htm